Every year approximately 4,000 Australians are diagnosed with cancer of the oesophagus or stomach (incidence of 1 in 6,500). This however is much lower than what is seen elsewhere in the world (such as Japan and Korea which have the highest incidence of approximately 1 in 2000). In Australia, this affects predominantly the upper part of stomach
Causes
Like cancer elsewhere, there are strong associations between cancer of the stomach and the following conditions
- Smoking
- Reflux (GORD)
- Chronic atrophic gastritis and intestinal metaplasia. This refers to a change or adaptation of the lining of the stomach that resembles the intestines in response to a number of stimuli such as
- Chemical irritation. It has been previously postulated that poor quality diets as seen in third world countries as well as diets rich in cured foods (pickled meat, fish and vegetables) was a source of nitrate compounds that are carcinogenic to the stomach. There has however not been any strong evidence from scientific trials to make these associations to date.
- Infection with Helicobacter pylori. This bacteria has been found to exist as a commensal (part of the normal bacterial presence in the stomach) and produces various toxins that have been found to be carcinogenic to the stomach specifically. A rapid biopsy test during a gastroscopy can determine the presence of this bacteria in the stomach and if detected warrants eradication with a course of specific antibiotics.
- Auto-immune disease where the produces antibodies against the stomach inducing damage (pernicious anaemia)
- Certain types of polyps in the stomach
- Certain hereditary conditions (genetic cancers here are less than 1%)
- Chronic ulcers can rarely turn cancerous.
Symptoms
The symptoms of gastric cancer can be vast, but attention should be sought in the event of developing
- Difficulty swallowing
- Upper abdominal pain
- Long standing nausea and vomiting
- Weight loss and or lack of appetite
- Haematemesis or vomiting up blood
- Heartburn or reflux
- A feeling of feeling full easily after a meal (early satiety)
Investigations
The initial investigation should be a gastroscopy (examination of the oesophagus and stomach with a flexible camera). This is the most sensitive test for detecting these cancers. During this test, a biopsy may be taken of the tumour to confirm the diagnosis and determine the type of tumour; this will help determine the best treatment, based on chemotherapy, radiotherapy and/or surgery.
Other tests can be supportive or provide additional information such as
- Barium meal (an XR of the stomach with swallowed dye)
- CT scan of the chest and abdomen
- EUS is an ultrasound examination of the lining of oesophagus or stomach with a specialized camera.
- PET scan is used to detect areas of distant spread of cancer
Treatment
The treatment of oesophageal or stomach cancer involves a thorough assessment along the lines mentioned above in order to determine the degree of growth or spread. This is done so that treatment can be tailored to the individual patient and based on best available evidence. This is arranged by a multidisciplinary team involving a Nurse, Dietitian, Surgeon, Oncologist, Radiologist and Pathologist.
In summary, treatment involves,
- Consultation with a dietitian to determine state of nutrition and how to overcome deficiencies or supplement nutritional intake during and after the treatment phase.
- Consultation with an Oncologist determines stage of disease and plan for any chemotherapy/radiotherapy, which may be before or after any surgery.
- Consultation with a Surgeon to determine stage of disease, and discuss arrangements for surgery and procedures involved.
- This may involve an initial assessment on the operating table (a minor operation) called a staging laparoscopy where an assessment is made of the state of disease to determine if it is localized to the oesophagus or stomach and has not spread.
- Standard treatment would involve a short course of chemotherapy prior to surgery. This has been shown in scientific trials to be more beneficial than surgery alone.
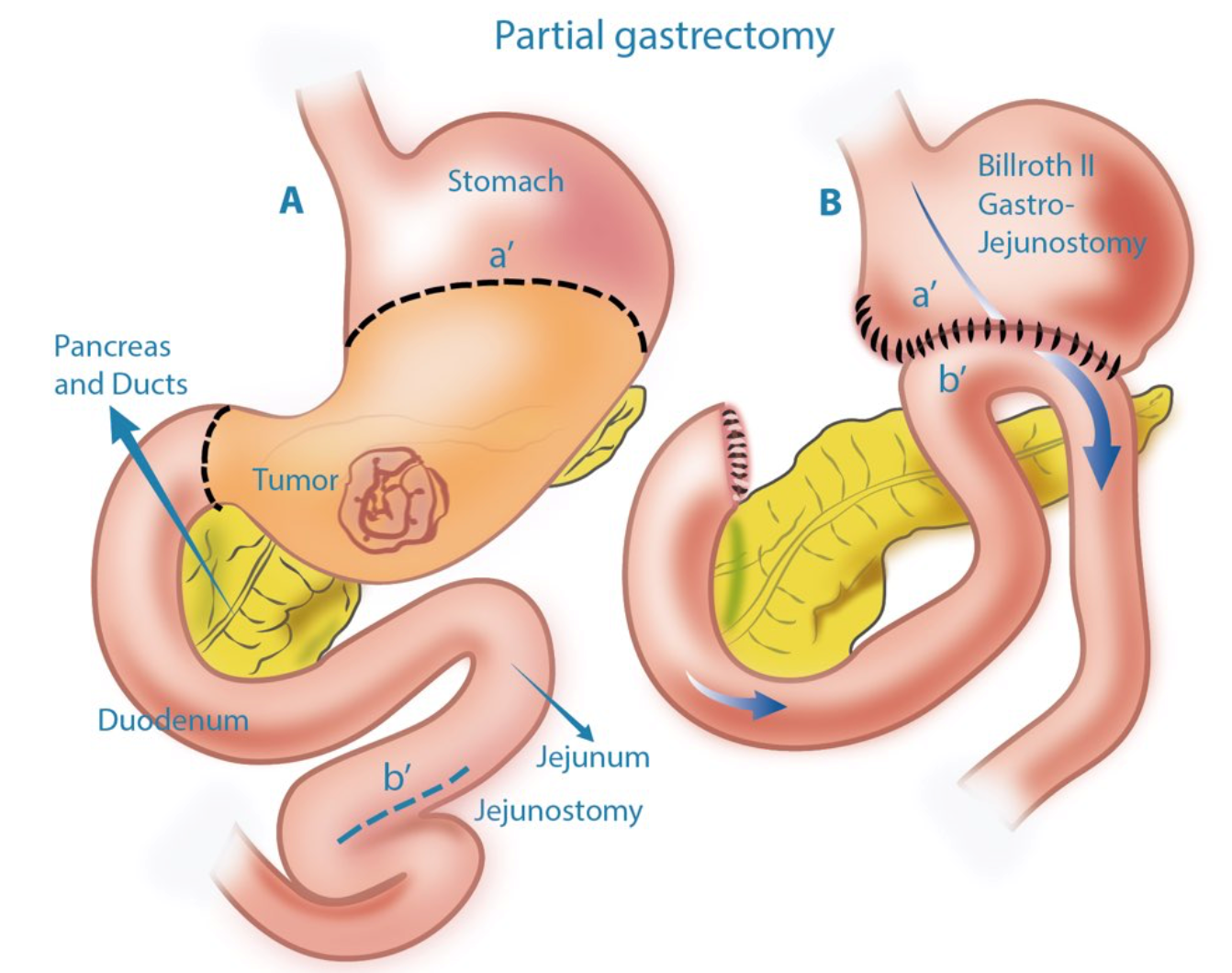
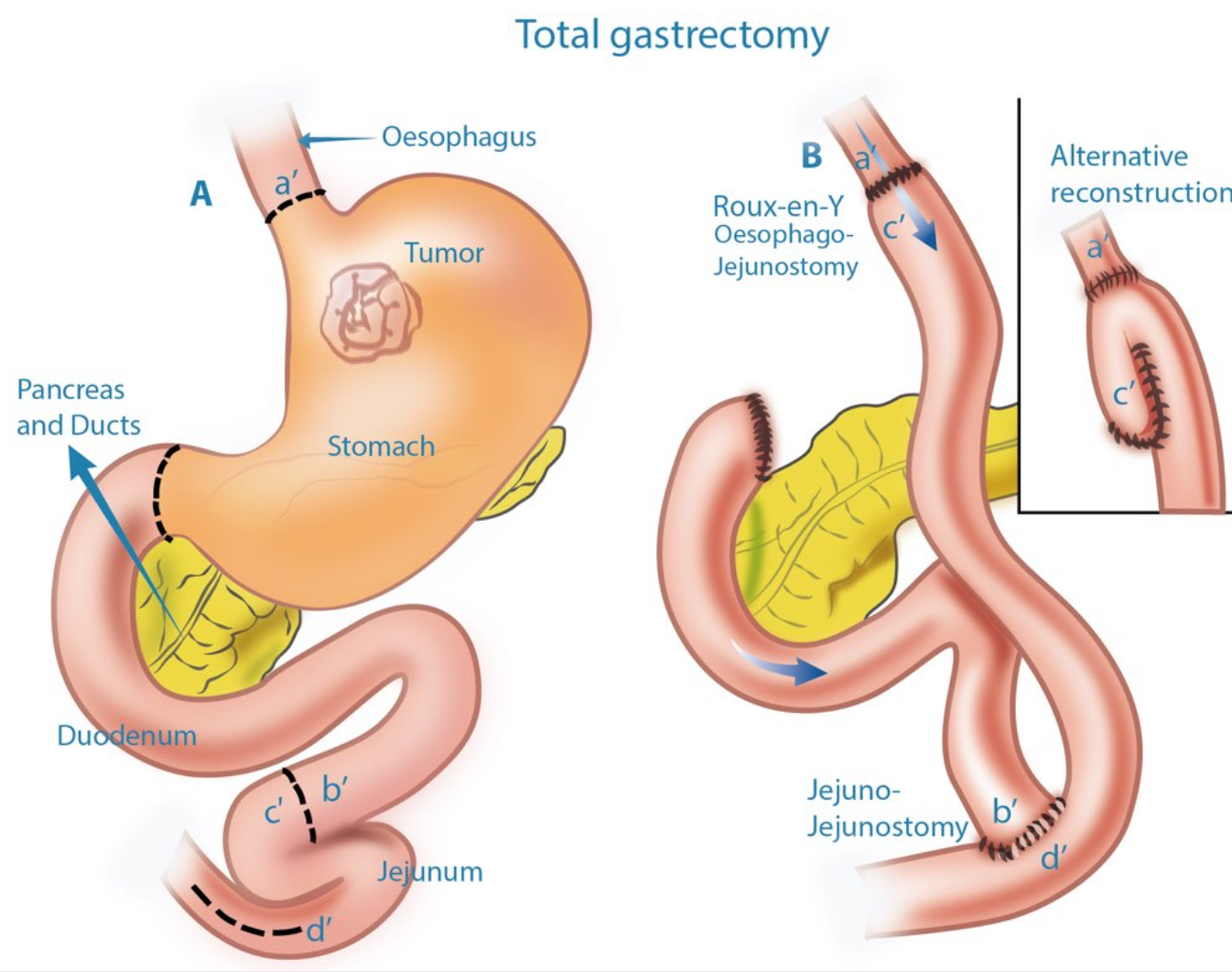
- Surgery, to then remove part or whole of oesophagus or stomach (as well as its surrounding glands) would then take place approximately 2 months later. Exact details of the surgery and the reconstruction involved can vary and should be discussed with the Surgeon.
Please understand that the information that is provided on this website is to serve as a guide only. This does, by no means, negate or alter the need for a full individual consultation and medical assessment.
I am text block. Click edit button to change this text. Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.