What is a Gastric Bypass?
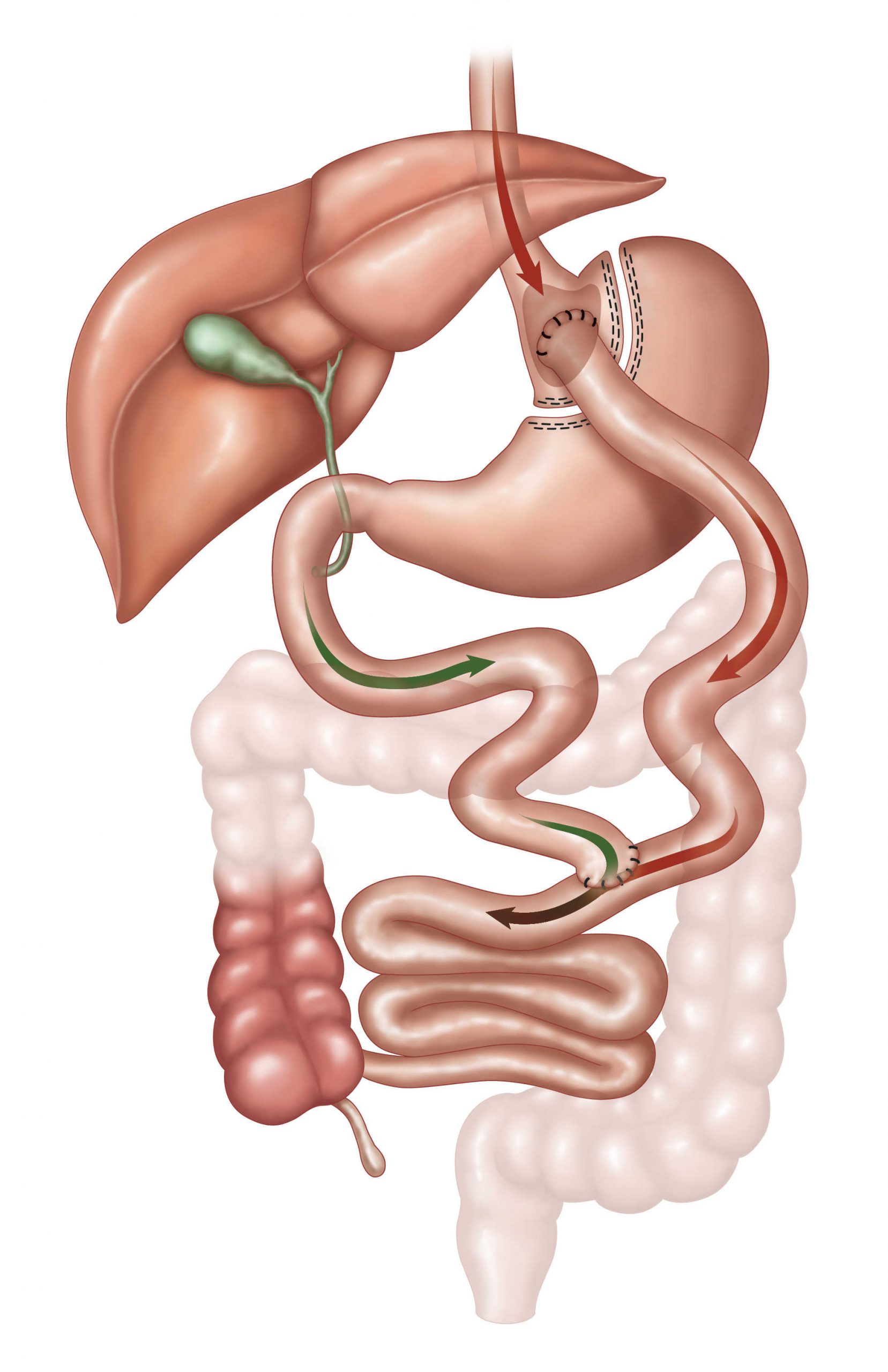
A Gastric Bypass procedure or RYGB (Roux-En-Y Gastric Bypass) is when the top portion of the stomach is divided to create a small gastric pouch or smaller stomach with a new opening. The smaller stomach is then joined to the jejunum (middle part of the small intestine).
This allows food to “bypass” the lower stomach/upper small intestine and move directly into the lower intestines. This reduces the amount of food that is tolerated, and also causes malabsorption by bypassing the first part of the small intestine, the duodenum. This effect is a result of both decreasing the length of the small intestine available for absorption of food, and alteration of gut hormone levels that occur when the first part of small intestine is bypassed.
It also has a specific effect on diabetes. In combination with weight loss, bypass triggers enhanced insulin function and the effect on diabetes can be dramatic with most studies reporting about 80% resolution of diabetes.
Variants of this procedure include the more recently described Mini Gastric Bypass-One Anastomosis Gastric Bypass (MGB-OAGB) where the intestine is not divided but simply attached to the upper stomach pouch. This has shown great promise in published studies. The benefits of this procedure have been described in terms of excellent weight loss, resolution of co-morbidities (at least equivalent to standard gastric bypass or Roux Y Gastric Bypass), but fewer bypass related problems such as internal hernias. There is also the added flexibility of being able to adjust the length of small intestine that is bypassed, to address further weight loss requirements or even rarely where weight loss has been excessive.
Other procedures such as SIPS (Stomach Intestinal Pylorus Sparing) or SADI (Single Anastomosis Duodeno-Ileostomy) surgery have been performed and provide for excellent weight loss but may require greater nutritional surveillance. These can be performed as primary or revision surgery options. Please discuss these options with your Surgeon as to suitability.
Both the Gastric Bypass and Mini Gastric Bypass (MGB-OAGB) can be completed Laparoscopically and Robotically.
Risks
Being the most complex of the operations, the operative risk is also higher. The main issue is leak from the staple from any of the joins or staple lines (3-5%).
Advantages
- Reliable, proven operation with consistent results
- Particularly good results seen in Insulin dependent diabetics
- Average 65-80 % EWL
Disadvantages
- Irreversible change to anatomy
- Greater nutritional surveillance required including blood tests every 6 months.
Please understand that the information that is provided on this website is to serve as a guide only. This does, by no means, negate or alter the need for a full individual consultation and medical assessment.